One day I was taking a break from swimming in the pool when the fellow in the next lane struck up a conversation. He told me how he had a heart attack eight months earlier. He was now swimming to stay in shape. Before his heart attack his doctor had told him that his lipids were perfect! Therefore, he did not watch what he ate and he would always go for that second slice of cheesecake! Now everything was different. Besides exercise he was now on a strict diet and watched everything he ate. Then he turned to me and said, “But my doctor said my lipids were perfect and I still had a heart attack. Can you believe it?”
Actually, I can. If you understand lipid metabolism you can imagine how such a thing is possible.
The above story illustrates some of the criticisms of the lipid hypothesis concerning CHD. But the Framingham Study showed us that the blood LDL cholesterol concentration was just the tip of one iceberg among many risk factor icebergs. And the process of CHD development is extremely complex and occurs slowly over many years. In fact, there are several biological avenues that can lead to increased atherosclerosis in the main coronary conduit arteries.
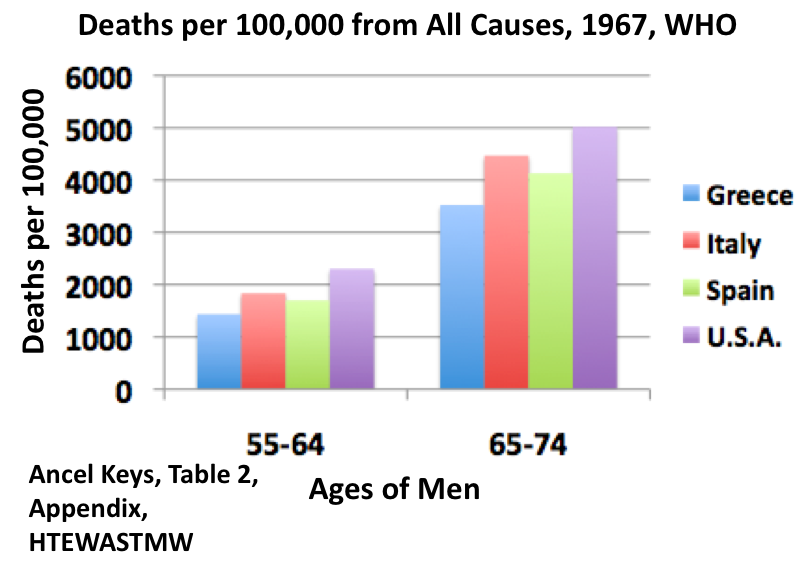
The experience of the Finns in East Finland after the realization that their diet was leading to increased CHD is probably the strongest data we have indicating that a high saturated fat diet, along with a diet low in plant materials, leads to high blood cholesterol levels and high CHD. When the Finns changed their diet, treated high blood pressure, and decreased smoking, their CHD rates decreased to 50% of the rates originally observed in the late 1950-early 1960s.
But the CHD rate still remained high and it is difficult to reverse atherosclerosis after someone has been eating a poor diet for many years. It is also the case that many other biological processes, besides high LDL cholesterol, are involved in the development of atherosclerosis.
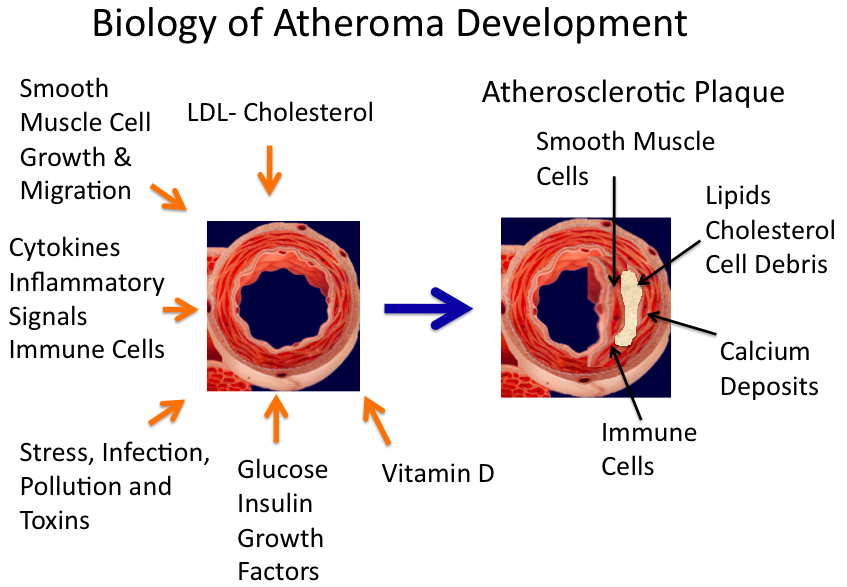
Let’s review some of the biological mechanisms that are now being investigated for their effects on the development of plaques in the coronary arteries. The following figure shows that there are many biological factors that affect the health of the artery. On the left is a spanking clean artery, and on the right is an artery that has an atherosclerotic plaque. The surrounding arrows on the left show that there are many biological processes that influence and stimulate plaque development.

LDL-cholesterol is just one factor. Another factor is the health of smooth muscle cells.
Smooth Muscle Cell Growth & Migration
Smooth muscle cells surround the endothelial cells, the sub endothelial space, and the internal elastic lamina that line the artery lumen (central area). Just like regular muscle, smooth muscle cells can either contract or dilate in order to change the area of the opening. For reasons that we do not understand, smooth muscle cells can turn proliferative and begin to divide. Then with the help of an enzyme called MMP-9, a protease that can chew through matrix, smooth muscle cells undergo migration and can move into the subendothelial space or even into the lumen of the artery.
Jason Lee Johnson. Emerging regulators of vascular smooth muscle cell function in the development and progression of atherosclerosis
Another factor involved in plaque development is the immune system and its powerful taskmaster, the inflammatory response, which is now considered a central mediator of atherosclerosis. As stated by one group of researchers, “Inflammation initiates, propagates, and complicates the course of atherosclerosis. A multitude of basic science work demonstrates this pathophysiological principle.”
D. Wolf; P. Stachon; C. Bode; A. Zirlik. Inflammatory mechanisms in Hämostaseologie 1/2014 63-71
An important aspect of the inflammatory response is the recruitment of immune cells to the location where the atherosclerotic plaque is growing. The reason for this is that the body wishes to repair the artery. But what really happens is that the immune cells will over react and damage the artery. The inflammatory response is thought to be behind the damaging effects of stress, infection, pollution and toxins.
Diabetes also has a very strong effect on coronary arteries. In fact, at each level of cholesterol concentration in the blood, diabetics have 4 times the rate of CHD compared to non-diabetics. This indicates that diabetes provides a very strong additional damaging effect on the artery above that provided by LDL-cholesterol. How diabetes increases heart attacks is a major research area in medicine.
There have been reports that low levels of vitamin D metabolites are associated with increased rates of CHD. Low vitamin D action may cause cells in the artery to lay down calcium phosphate, thus leading to the calcium build up observed in advanced plaque regions. Therefore, the extra levels of sunshine that people in the Mediterranean area receive the year round may increase vitamin D production in the skin. This would lead to greater activity of vitamin D dependent processes and cause the artery to be healthier, thus contributing to their lower rates of CHD. This is another reason why the intake of fish, which is high in vitamin D, may be protective against CHD.
Eva Kassi, Christos Adamopoulos, Efthimia K. Basdra, Athanasios G. Papavassiliou. Role of Vitamin D in Atherosclerosis. Circulation. 2013;128:2517-2531.
But why can’t I eat that second slice of cheesecake if my lipids are perfect?
The digestion and absorption of fat in the diet is extremely efficient, with greater than 90% of the fat consumed being rapidly absorbed and transported throughout the body for use or for storage in about 5-6 hours after a meal. This high efficiency and high capacity is evolutionary beneficial. And it also explains why your cousin didn’t collapse and die on his way home after he went to an “all the steak you can eat” restaurant and ate three 21 ounce steaks. The body can handle this amount of fat occasionally. Large intakes of nutrients, including fat, occurred throughout history when hunter-gatherers made big kills of animals after times of relatively low food availability.
Over flow of fatty acids in the post-prandial state (after a meal) – the work of Dr. Elizabeth Parks
We now realize that very high amounts of saturated fatty acids can lead to fatty acid toxicity, which is often the result of damaged mitochondria, the power houses of the cell. Repeated intakes of high fat diets may lead to sick or diminished mitochondria in both smooth muscle cells and in the cardiomyocytes, the main cell in heart muscle.
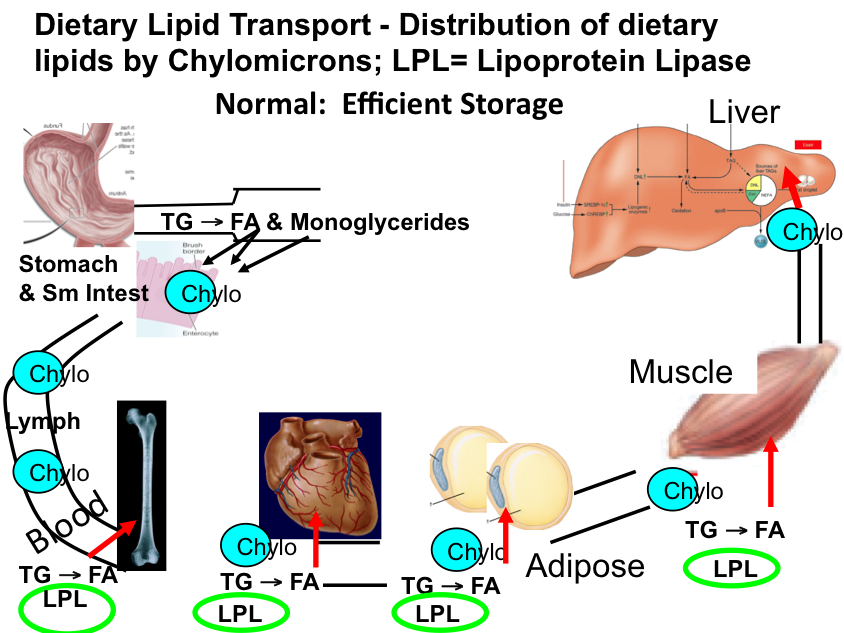
An example how this might occur has been put forth by Dr. Elizabeth Parks. For the past 10 years Dr. Elizabeth Parks has carried out the most exciting and informative studies on fatty acid metabolism in humans. She showed how both dietary and stored fat contribute to the free fatty acids that permeate throughout our bodies at every second of the day. Most recently she has documented fatty acid spillover after meals containing fat. Fatty acid metabolism is explained more thoroughly in the next chapter, but I wish to cover fat absorption from the diet right now. The figure below shows how fat is absorbed from the small intestine into the blood and how it is then distributed throughout the body for storage or use.
Lambert JE, Parks EJ. Postprandial metabolism of meal triglyceride in humans. Biochim Biophys Acta. 2012 May;1821(5):721-6
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3588585/

Fat is digested in the small intestine and is taken up by intestinal cells and packaged into a special lipoprotein called a chylomicron (Chylo). Chylomicrons are transported in the lymph and are dumped into the blood at the thoracic duct. Once the chylomicrons enter the blood they travel to peripheral tissues where an enzyme called Lipoprotein Lipase (LPL), which is on the surface of the vessels, traps the chylomicrons and cause hydrolysis of the triglycerides to free fatty acids. Through a mechanism that is not understood, these fatty acids enter the various tissues, where they are used for energy (bone marrow, muscle) or where they are stored (adipose tissue, aka fat cells). After permeating through the body what ever is left of a chylomicron particle is taken up by the liver. The most amazing thing about this process is its efficiency and speed; the half life of a chylomicron particle is five minutes.
In the second figure is a situation where there are much greater numbers of chylomicron particles in the blood and the tissues are not processing the fat fast enough. Therefore, there is fatty acid spillover into the blood and the fatty acids go to both the liver and the heart. The heart uses fatty acids for energy but it doesn’t have the ability to store them. Therefore, excess fatty acids cause damage to the mitochondria of the heart. The damage is probably not significant in the short time, but after many years of this abuse, there can be loss of active cardiomyocytes, the work horses of the heart. There is also increased proliferation of smooth muscle cells that cause plaque growth.

Dietary fat that is adsorbed into the blood has to be efficiently stored in adipose or oxidized in peripheral tissues like muscle. If not, there will be spillover into the free fatty acid pool in blood and this could make its way to the heart. Conditions that exacerbate the spillover are lack of exercise, diabetes, and very large fat meals. So in addition to bringing in those extra kcal, that second piece of cheesecake may be damaging your heart mitochondria or causing plaque build up.
The blood lipids that your doctor measures are levels of lipids that are in your blood in the fasting state. But all of the above happens after you eat a meal. Therefore, your fasting blood lipids can be perfect, but you can be doing yourself harm by eating a consistent high, saturated fat diet.
Remember, humans needed to process huge amounts of fat after that successful hunt, so occasionally, it is OK to eat that first piece of cheesecake!