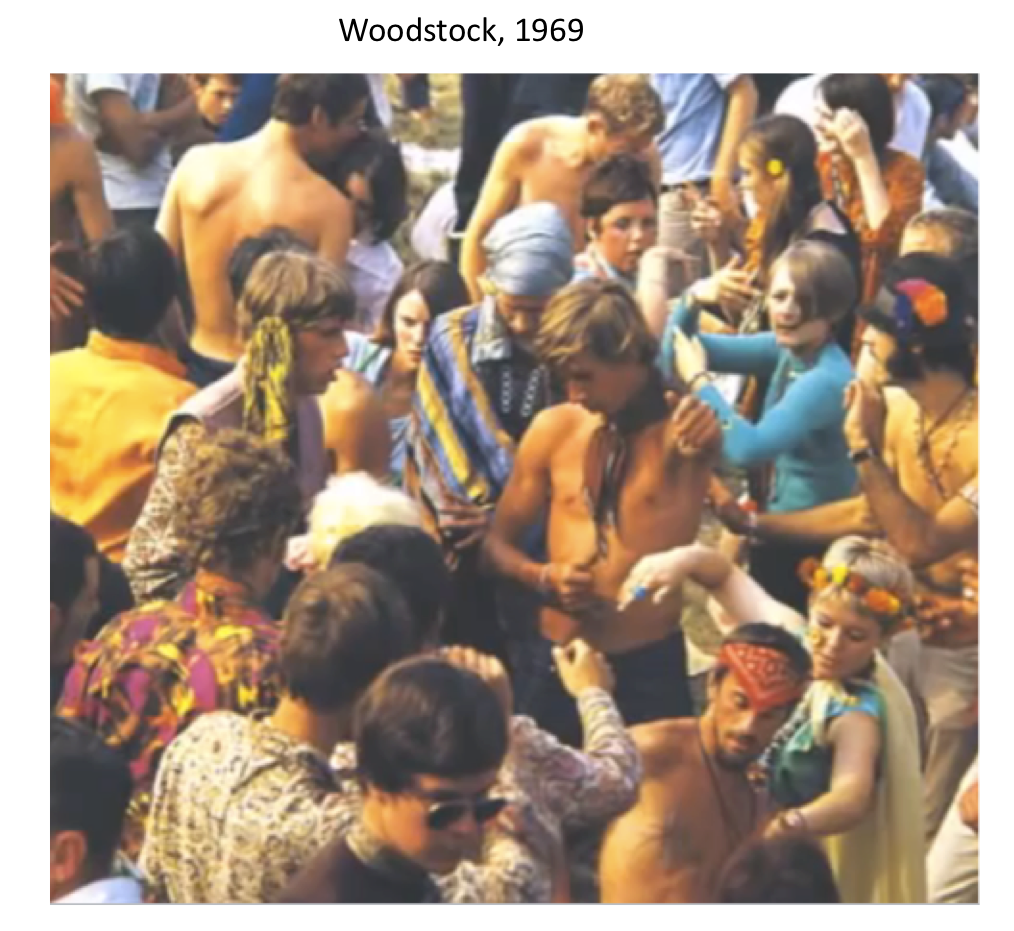
If any of you wish to remember how thin people were back in 1969, or if you are too young and wish to see this for the first time, please look at the movie “Woodstock” on YouTube (turn down the sound if you do not like rock & roll!; also, don’t look if you are upset by nudity, even if it is for science!). You will be absolutely amazed how thin teenagers and young adults were back then. Of course, you will see some heavy people, too (but very few), as there have been heavy people in most generations (probably because it is an evolutionary survival mechanism). The following are collages of screen shots taken from the Movie, “Woodstock.” But to get the full effect, you must go look at the movie to see how thin people were in 1969!



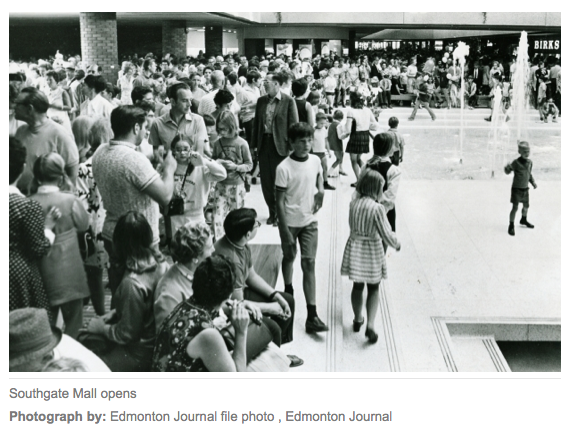
Shopping Mall in 1970:

Shopping Malls in 2013:


As someone who was very heavy as a child, I was happy to find this shot of me in college. The photograph below shows me with my roommates in our senior year (1976) of college at SUNY-Binghamton. We are outside of our house reenacting a famous album cover. I am the first in line and I was thin through the last portion of high school and all through college because I changed my eating habits and became very active, including backpacking throughout the entire western US when I was just nineteen years old.

Life before computers and obesity
Although I did not make it to Woodstock, I remember life at the time and how different it was from today. I was 15 years old in the summer of 1969 and still in high school. I lived in Brooklyn and city life was all I knew. In order to go to high school, I walked three long blocks up a steep hill and caught a bus to Flatbush Avenue, and then I transferred to a subway for the remaining trip. If I was lucky, I made it in about an hour.
Later when I went to college, I walked about twenty minutes from my dorm to the classroom buildings. When an exam was given that involved math, I needed to use a slide rule to perform calculations because hand calculators were not available yet.
And then in graduate school, when it came time to write my Ph.D. thesis, I needed to use a pencil to write out the chapters in the day and then at night I struggled typing my thesis on a typewriter. The Apple IIE was just becoming popular in the early 1980s (Data on computer availability will be presented in a later Chapter).
Because computers and ubiquitous fast food were not yet available, what was life like growing up in the 1960s and the early 1970s?
Grocery Shopping Before Obesity
I remember many things about my early life that pointed to a very active childhood. One example is that my mother did not drive, and therefore, when we went to the supermarket, we took out the grocery cart and pulled it behind us. We needed to walk 2 and ½ flat blocks and then we headed down a long steep hill. I hated walking down that hill because I knew that later on we would need to walk back up it. We walked another 3 blocks and came to our local A&P supermarket. We went in, attached our cart to the grocery cart, and then proceeded to go down the first short aisle on the left side of the store. We then moved to the next aisle, which was much longer. After grabbing groceries from the middle aisle, we went all the way to the rear of the store to cross over to the third aisle.
After making the turn, you then went down the final long aisle to the check out counters. That was it – 3 aisles in all! The A&P was stocked with staples but with little else. This small A&P had a dairy section, a bakery section, a frozen food section, a canned goods section, but few others – not the dozens that are found in modern mega supermarkets today. And one thing our small A&P had very little of were processed foods.
One of my greatest fears as a child (I still have dreams about this even today!) was being asked by my mother to go back and get something that we had forgotten to put into the grocery cart. I could not go back up the last aisle we had come down because the flow of traffic was only one way and I would be run over by the other shoppers. So I needed to slip under the bar that separated the checkouts from the first aisle and then I would navigate back through the entire store to get the needed item. I then needed to weave through the remaining aisles to get back to the check out. The smallness of the A&P made only one-way traffic possible.After paying we would load the brown bags into our pull shopping cart and start the walk back home. And yes, we needed to climb that long hill to get there. I will always remember the pain of going up that hill as a little boy!
Having a child help make the family meal at home
Today as I write this in 2013, it has been reported by several researchers that currently 40 to 50% of money spent on food is spent eating outside the home (I’ll present this data in later chapters). This is an astonishing figure because as a child growing up, my family went out to eat infrequently – maybe twice a year. And usually this was for a special occasion, such as a birthday. We essentially never went out to eat in a restaurant. No one that I knew at the time did. From this we can infer some basic facts. First, when I was a child in the late 50s and early 60s, at least where I lived, most food was consumed in the home, and therefore, most food was prepared in the home.
In order for this to occur a spousal unit needed to be at home in order to shop, prepare, and serve the meals. When I was young, this was my mother, who never worked outside the home. And this was possible because the economic paradigm at the time allowed for one wage earner to support a family, and this allowed one spouse to remain at home.
This basic operational model had other major effects on family life. Since a spousal unit was always at home, the smaller kids could be watched by a parent and taken along on errands and visits around the neighborhood. Being home, a child could help the parent in the kitchen with elementary tasks. This was an excellent opportunity to learn how to cook at a very young age. In an extended analogy, this was not unlike a child following around a mother or father to learn how to gather and prepare food in a Hunter-Gatherers’ village.
If a child in a village can learn helpful family tasks, why not a child in a modern American home? In fact, this was how I learned to cook, and probably where I carried out my first chemistry experiments. From a very early age I knew how to wash vegetables, peel potatoes, mix ingredients in a bowl, and prepare meats. I was also the person who set the table and put drinks from the refrigerator on the table. After doing this many times – it becomes second nature, like learning a language. When I later went to college it was an essential survival skill to make meals in my apartment. And like learning to ride a bike, cooking is something that you never forget how to do.
Shopping in Manhattan Before the Shopping Mall
When my mother took me with her on a shopping trip, it was an opportunity to eat outside the house, but not at a fast food restaurant, because they did not really exist at the time. My mother would take me with her on the subway into New York City (aka Manhattan). She would shop in midtown at Macy’s or Gimble’s near Herald Square. Usually we ate in a department store cafeteria. But occasionally, we ate at the Horn & Hardart automat in midtown. The automat was a flashy, bright cafeteria style restaurant where there was a large sitting area in the center of walls of shining doors with little windows.
This was such an amazing experience and I always wondered whether there were robots in the back that made the food. Actually there were hard working food service workers but we couldn’t see them. My mother gave me the coins to put into the slots and after putting the money in you turned a knob and then you could open the door and take out the dish with the food. I would eat the baked beans or the macaroni and cheese, both standards at the automat.
My mother would always eat the creamed spinach or a fish cake. This trip to the automat made the long subway ride and the walking through crowds and busy traffic of Manhattan streets bearable. At least there was something exciting to look forward to while my mother shopped. To this day I hate shopping of any kind. I remember having to wait while my mother searched for clothes for my four sisters. She never bought anything for herself. And my feet – they would hurt and sweat the entire time. I can still feel them! After the trip to the store and lunch we headed back home on the subway.
I would fall asleep to the back and worth motion of the subway cars. At our stop my mother would wake me up and then we climbed our way to the street where we would find ourselves near the A&P supermarket I described earlier. Once on the sidewalk we walked back to our house, walking up the same hill that I dreaded when going to the A&P. Finally, we were home!
How was that trip into Manhattan on the subway different than the trip to the mall by car today? We walked at least a half-mile to the subway stop. After descending the stairs we needed to wait for the train. In Manhattan we had to walk up the stairs and then over from 6th Avenue to Herald Square. And on the way back everything was reversed. Today, in most cases people drive to the mall, park their cars, and walk in. They stay for several hours, about the same period of time as we stayed on our shopping trip. They walk through the mall but do not exercise anywhere near as much as we did taking the train. Then they walk the short distance to their cars and get in and drive away. Our eating experience in Manhattan was different than most eating experiences today.
By eating in a cafeteria we obtained basic food to eat and it did not consist of a burger and fries or another popular fast food. Some common cafeteria foods at the time were a sandwich on toast, tuna fish on a green leaf salad, soup and crackers, a meat with vegetables entree, and don’t forget a bowl of Jello or pudding for dessert. Drinks were only 8 oz at most. Who would want to drink a 20 oz drink? We were use to eating normal size means for normal sized people (as least 95% of us were normal sized!).
Once home my mother would start supper and we would eat our dinner at home like we did every other night. But it was certainly a treat to eat in a cafeteria or the Automat. We did eat out, but we also walked a great deal and probably burned all those kcal up.
The one exception – Brooklyn Pizza
There was one exception to the above. If I am to be honest, we did spend money on food made outside the home. After all, Brooklyn pizza is famous throughout the US. Every so often when my mother needed a break, we would order pizza from the local pizzeria. We would call in our order and my father would drive and pick the pizza pies up. This was always a treat for us. Also, on some occasions, when I was older and I was out at a boys club meeting, I would stop on the way home at a pizza place to get a slice. I remember that the price of a slice of pizza was 15 cents. And I remember quite vividly that the price of a ride on the subway was always the same price as a slice of pizza. At the time it was also 15 cents for a ride on the subway. Today in 2013 the price of the subway is $2.25 and the slice of pizza runs from $1.75 to $2.50 depending on the location of the pizza shop. So the relationship is holding up pretty well.
My first fast food experience
It was in the summer of 1969 and some of my older friends were going to go to the Woodstock Music and Art Fair. I asked my mother whether I could go with them. She said definitely not. After all, I was only fifteen years old and I had only one year of high school behind me. My mother had a better idea. I could fly down to Atlanta Georgia and spend a week with my two sisters, Rita and Jeanne. This coincided exactly with Woodstock. So I flew down to Georgia and I do not have many memories of the trip. However, the one thing that I do remember perfectly is walking across the street from Rita’s apartment and eating a Whopper at a burger king fast food restaurant.
The experience is indelibly etched into my mind. The charcoal broiled burger, the lettuce, tomato, pickle and ketchup. And the mayo on the lettuce. All enclosed in sesame seed bun. How delicious. High salt, high fat, and I am sure there is sugar somewhere in the concoction. The combination of flavors was a taste orgy to my brain. To this day I remember that experience and sometimes crave a Whopper sandwich. At a moment’s notice I will need to go out and find a Burger King place. So there was something in that sandwich that caused a pathway of neurons to be laid down in my brain. And whenever there is activity in that pathway of neurons, I need to go out and find and eat a Whopper! Nothing else will satisfy me.
Driving to College Before obesity – difficult to eat on the way
After high school I went to college in upstate New York. Once a week I tried to call home, usually on the week end. There was one telephone booth and if you did not wish to wait on a long line, you needed to get up early on a Saturday morning to make a call. There were no private telephones or cell phones.
After trips back home or at the beginning of a semester, I would drive up to college either with a friend , or later on by myself when I had a car.
When it was time to drive back to college I packed the car and took off about 10 am. I was driving from Brooklyn to Binghamton NY and I had eaten breakfast but did not pack a lunch. After navigating the roads out of New York City, I was on the NY State Thruway and would soon take route 17 to head northwest to Binghamton. It was getting near 12 noon and I was a little hungry. I just put it out of my mind and made a note to stop at the Roscoe diner in about an hour. The traffic was fairly light and I made good progress. I exited at Roscoe and pulled into the Roscoe diner’s parking lot.It was packed and I knew immediately it would be a long wait to get seated and then eat lunch.
I walked in and when I heard it would be 40 min wait before I could sit down, I just turned around and got back into the car. I put my hunger away and continued on my trip to Binghamton. Several hours later when I arrived at my apartment, I looked in the refrigerator. There were a few very suspect food items in there. I walkeddown to the local grocery to buy some bread and cheese. I made myself a sandwich and drank some milk. I was finally not hungry. It wasn’t a big deal. It was 1974 and it was typical to make the drive between NY and Binghamton without eating. After all, there were few places to eat along the way. There were certainly no fast food places to stop. At least none I can remember. And not seeing a restaurant at every exit didn’t coax me into stopping and eating. Not having an easy place to stop and eat was very common at this time before the appearance of the obesogenic environment in the United States.
Conclusions
The conclusions from the above stories is that it was necessary to perform energy intensive physical activities in order to carry out everyday life events. Even the process of making dinner in the home required work that helped burn kcal in the preparation of family meal. Today, even in some cases if you still need to perform physical activities in the daily routine, it is easy to stop and consume a fast food meal. Why the pre-1980s was less obesogenic revolves around the sum of every day activities that required energy expenditure and the inability to quickly stop and eat a high kcal fast food meal.